×


Normally, in both bone fractures, the simpler fracture will be approached first, and preliminary fixation undertaken. Fixation of the fractures involving both bones proceeds as follows: Reduction and preliminary fixation usually starts with the ulna. Reduction and definitive fixation of the radius.





Recovery. Supracondylar humerus fractures often heal within 4 weeks from start of treatment (either casting or surgery). After your child's cast is removed, it may take 4 weeks for them to be able to move their elbow normally. If your child had pins in their arm, they will get a sling or removable long arm splint.




The forearm fractures are usually managed by surgical fixation, including closed or open reduction and internal fixation. Open reduction helps achieve anatomic reduction, stable fixation, and an early range of motion, thereby enabling patients to return to their pre-injured state as early as possible.



Fracture of the distal radius is a common clinical problem. Displaced fractures are usually reduced using closed reduction methods, which are non‐surgical and generally comprise traction and manipulation. The resulting position is then stabilised, typically by plaster cast immobilisation.



This option is usually for fractures that are considered unstable or can’t be treated with a cast. Surgery is typically performed through an incision over the volar aspect of your wrist (where you feel your pulse). This allows full access to the break. The pieces are put together and held in place with one or more plates and screws.
In certain cases, a second incision is required on the back side of your wrist to re-establish the anatomy. Plates and screws will be used to hold the pieces in place. If there are multiple bone pieces, fixation with plates and screws may not be possible. In these cases, an external fixator with or without additional wires may be used to secure the fracture. With an external fixator, most of the hardware remains outside of the body.
After the surgery, a splint will be placed for two weeks until your first follow-up visit. At that time, the splint will be removed and exchanged with a removable wrist splint. You will have to wear it for four weeks. You will start your physical therapy to regain wrist function and strength after your first clinic visit. Six weeks after your surgery, you may stop wearing the removable splint. You should continue the exercises prescribed by your surgeon and therapist. Early motion is key to achieving the best recovery after surgery.

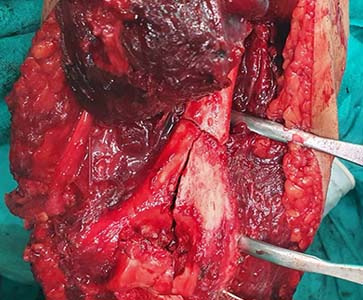
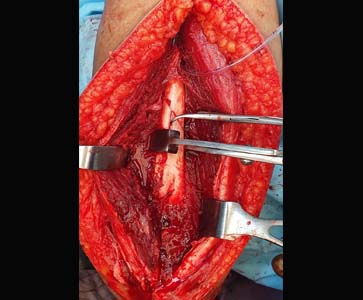
This is the procedure most often used to treat distal humerus fractures. During the procedure, the bone fragments are first repositioned (reduced) into their normal alignment and then held in place with plates and screws attached to the outside of the bone.






An elbow fracture can occur for various reasons, including a fall, direct impact to the elbow, or overuse. The severity of the injury can vary from a minor hairline fracture to a complete break in the bone. The treatment plan will ultimately depend on the medical diagnosis.
Surgery may be needed in some, but not all, cases. Read on to learn about the nonsurgical and surgical treatment options.



An elbow fracture can occur for various reasons, including a fall, direct impact to the elbow, or overuse. The severity of the injury can vary from a minor hairline fracture to a complete break in the bone. The treatment plan will ultimately depend on the medical diagnosis.
Surgery may be needed in some, but not all, cases. Read on to learn about the nonsurgical and surgical treatment options.

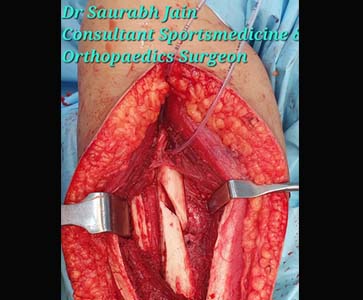

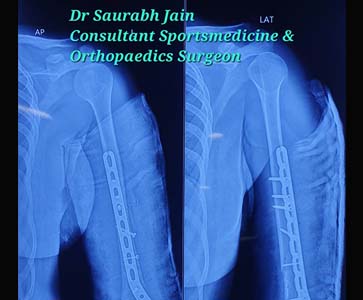

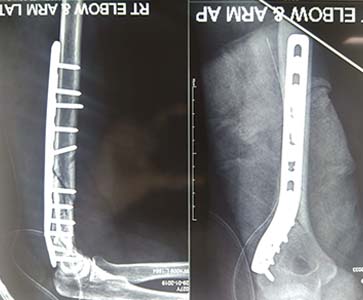
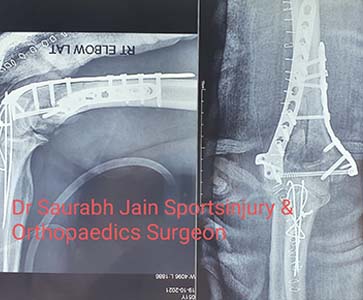
Humeral shaft fractures are common fractures of the diaphysis of the humerus, which may be associated with radial nerve injury.
Diagnosis is made with orthogonal radiographs of the humerus.
Treatment can be nonoperative or operative depending on location of fracture, fracture morphology, and association with other ipsilateral injuries.



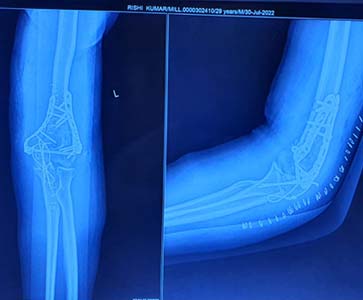
A galeazzi fracture is a distal 1/3 radial shaft fracture with an associated distal radioulnar joint (DRUJ) injury.
Diagnosis can be suspected with a distal radius fracture with widening of the radioulnar joint on AP wrist radiographs and volar/dorsal subluxation of the radioulnar joint on lateral wrist radiographs.
Treatment is generally ORIF of the distal radius followed by assessing the stability of the DRUJ which may be warrant subsequent immobilization, DRUJ pinning or ORIF of the DRUJ.


Humeral shaft fractures are common fractures of the diaphysis of the humerus, which may be associated with radial nerve injury.
Diagnosis is made with orthogonal radiographs of the humerus.
Treatment can be nonoperative or operative depending on location of fracture, fracture morphology, and association with other ipsilateral injuries.







